In 1995, one of healthcare’s most notorious failures made headlines: a Florida surgeon amputated the wrong leg of a patient named Willie King. The surgeon, Dr. Rolando Sanchez, became the face of hospital error almost overnight. The public and media demanded to know: How could such a catastrophic mistake happen?
In response, the state health agency took decisive action, suspending Dr. Sanchez’s license and labeling him an “immediate and serious danger to the health, safety, and welfare of the public.” This reaction stood in stark contrast to Florida’s backlog of nearly 50 other malpractice complaints at the time. But the Willie King case would be different. This time, someone would be made an example of. Human error would not be tolerated.
Don’t miss our free webinar, 30 Years Later: How Lessons from the Willing King Wrong-Site Surgery Apply Today, on August 15, 2025.
From Blame to Breakdown: How the System Failed Willie King
As human beings, we have an instinctive tendency to assign blame, especially when the outcome is severe. It’s a well-documented cognitive bias: we are quick to judge past actions because we already know their consequences. In this case, Dr. Sanchez was the last person to “touch” the patient, so fingers pointed to him.
But the reality was far more complex. This tragic story starts long before Dr. Sanchez entered the operating room.
On February 20, 1995, 51-year-old Willie King—a diabetic patient suffering from circulatory disease—was scheduled to have a foot amputated. During the surgery, Dr. Sanchez realized too late that he was operating on the wrong leg. The operation had already progressed past the point of reversal. Given the gravity of the error, public reaction was swift.
How could a licensed surgeon make such a catastrophic mistake? He must be incompetent, careless, or complacent!
But as with every serious incident, a deeper look tells a different story, one that goes beyond individual actions and exposes the system-wide breakdowns that made the error possible. In fact, one of the first things we learn when we begin to analyze the incident is that Dr. Sanchez believed he was removing the correct leg.
5-Why Analysis: A Simple Start to a Complex Failure
Our initial analysis uses a 5-Why Cause Map™ diagram to trace the basic chain of events that led to the wrong-site amputation. We now learn that Dr. Sanchez thought he was removing the correct foot. Why? Because the wrong leg had already been prepped for surgery before he entered the operating room—a mistake triggered by a prior scheduling error.
Wrong-Site Amputation 5-Why Cause Map™ Diagram

This map is accurate, but it only represents a simple, partial explanation of the causes that produced the incident. If our analysis stops here, we risk shifting the blame from Dr. Sanchez onto someone else, like the scheduler. This 5-Why provides a baseline understanding, but it also highlights what’s missing from our analysis and raises questions such as:
- How did the scheduling error lead to the wrong foot being amputated?
- Why didn’t we recognize that the “good” foot didn’t need to be removed?
- Shouldn’t we have caught the error before the procedure was performed?
Where the Process Broke Down (Again and Again)
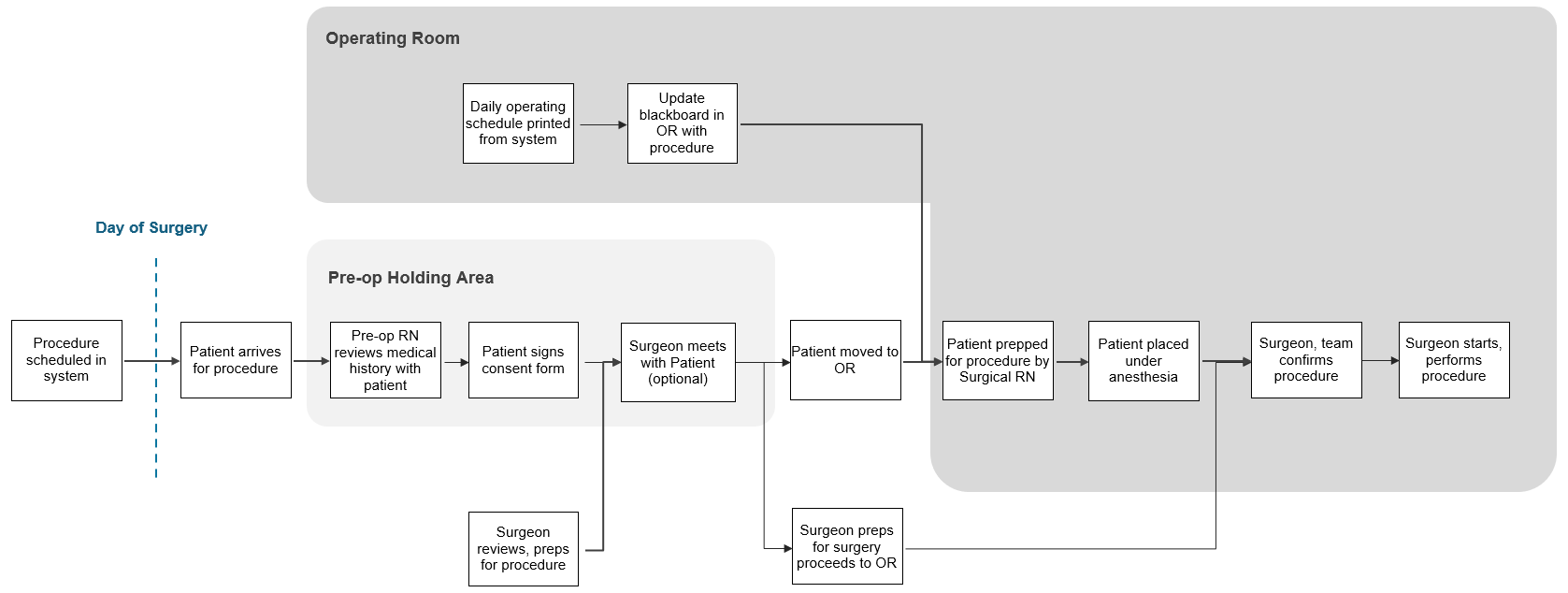
To understand how this error reached the patient, we need to shift focus from who made the mistake to where the process failed to catch it. That’s where process mapping comes in. Just like a Cause Map diagram facilitates discussion around the causes, a process map facilitates the discussion around the work and how it’s supposed to be done. In this case, building a process map for a typical surgical workflow reveals the steps involved as well as opportunities to detect and prevent the error.
Surgical Procedure Process Map
Through the process map, it becomes clear that the error didn’t slip through just once. It passed through multiple checkpoints: scheduling, documentation, and pre-op prep to name a few. In total, we can identify at least seven steps that were not effective.
Surgical Procedure Process Map with Process Breakdowns
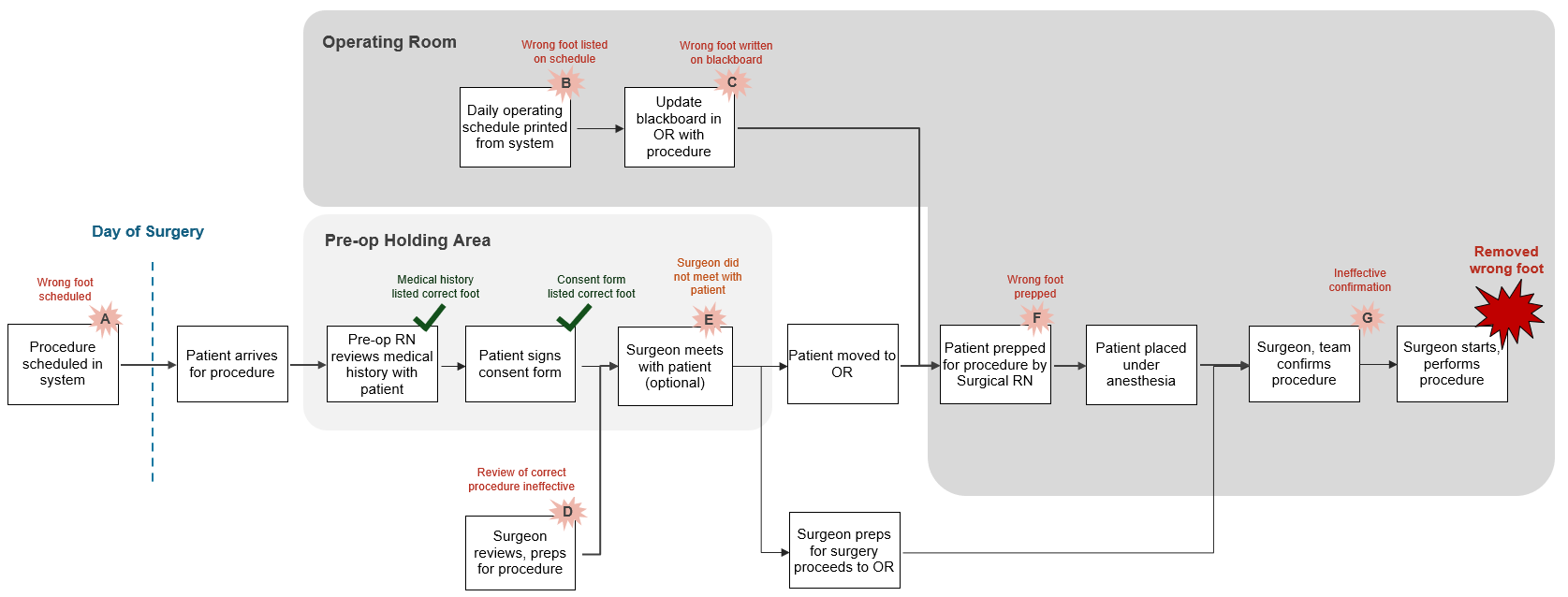
This was not a single-point failure. Each of these steps is a potential control point—an opportunity for the system to catch the error. When multiple checkpoints fail, we don’t have a “people” problem. We have a “system” problem.
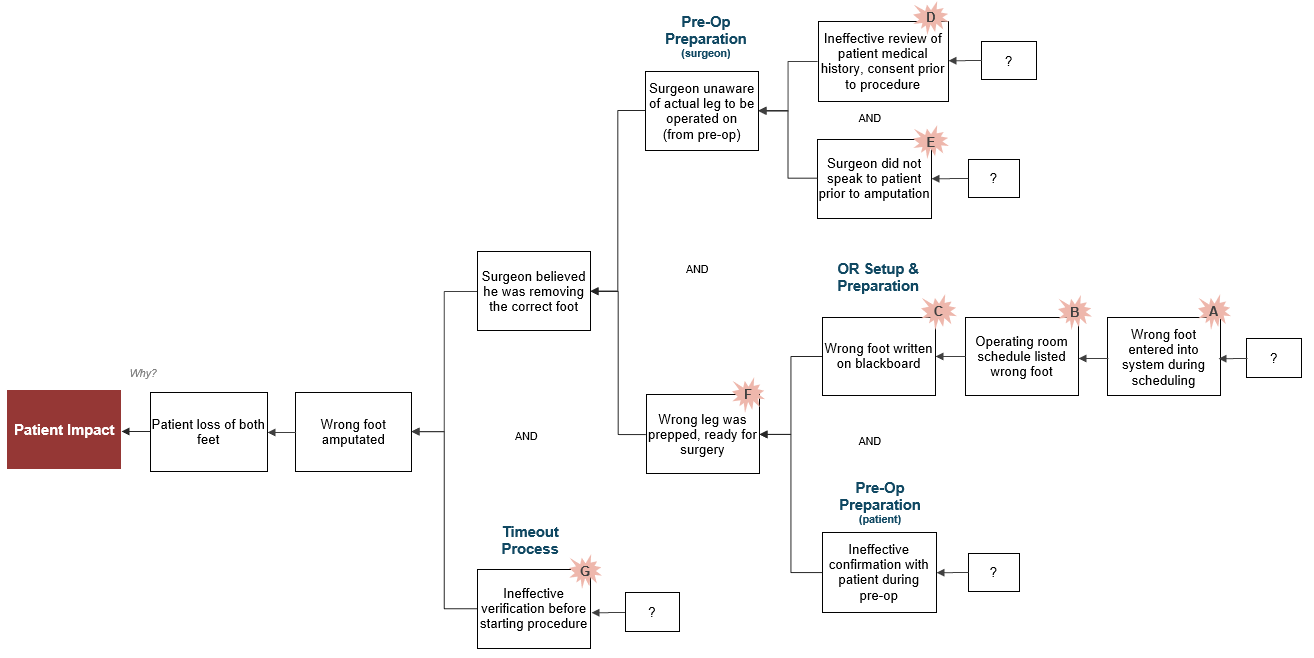
Expanding the Cause Map™ with Process Insights
Armed with a better understanding of the process, we can now return to the Cause Map diagram and expand it meaningfully. The analysis shows that:
- The scheduling error was only the starting point.
- Documentation issues, ineffective verification processes, and inadequate safeguards were all required as well.
- Each ineffective step was a missed opportunity to catch and correct the mistake.
- Controlling any one of these causes would have prevented the tragic outcome.
This approach shifts the focus away from blaming individuals and toward fixing broken systems.
Wrong-Site Amputation 13-Why Cause Map™ Diagram
What We’ve Learned and Put into Practice Since
In the decades since this event, healthcare has made major strides in reducing wrong-site surgeries, thanks in part to lessons learned from this case. Today, several widely adopted safeguards are in place.
- Patient involvement: Patients now mark the surgical site themselves with a Sharpie.
- Pre-surgery consultation: Surgeons are required to meet with patients during pre-op to review the procedure and confirm the consent form.
- The “Timeout”: A final pause before incision is now standard practice, where the surgical team confirms the patient’s identity, the procedure, and the surgical site. Even if multiple errors are made earlier, this last line of defense can prevent serious harm.
Each of these practices is designed to catch errors before they reach the point of no return. Importantly, none of these preventative measures rely on perfect human performance. Instead, they acknowledge human fallibility and build process layers that account for it.
Manage by Process, Not by Blame
The Willie King case remains one of the most powerful reminders of what we miss when we focus on people instead of the process. It’s a cautionary example—not just about surgery, but about how we approach error in any complex environment.
Blame may feel satisfying and fair in the moment. But it often reveals our lack of understanding, and it ultimately solves nothing. To actually mitigate risk we must understand the specific causes of our incidents and use them to improve the system itself. That means designing processes that help people succeed, even when they make mistakes.