
A medication error is defined as "any preventable event that may cause or lead to inappropriate medication use or patient harm while the medication is in the control of the healthcare professional, patient, or consumer,” according to the National Coordinating Council for Medication Error Reporting and Prevention. In this medication error case study, a patient was given the wrong medication, a chemotherapy pill instead of an antibiotic pill, for almost two weeks. It may be hard to imagine, but the patient was OK and suffered no adverse side effects from the error. In this week’s blog, we use the Cause Mapping® method to reveal the breakdowns in the work process that resulted in this mistake and near miss for the patient.
What Happened?
A non-certified nurse arrived at work on the oncology unit and began their day as normal. As they were making their rounds, they arrived at a patient who needed their chemo medication. The non-certified nurse located a certified nurse and asked for help in completing the medication administration process.
For background on the chemotherapy medication administration process, prior to administering a chemo medication, an independent verification of the original order in the patient’s chart must be compared against the actual medication delivered to the patient by a chemotherapy-certified registered nurse (RN). This verification is to be performed every time a medication is administered, i.e., twice a day for multiple days in a row. If a non-certified RN happens to be caring for the patient when the medication needs to be given, then that non-certified RN must find a certified RN to complete the process.
Prior to this day, the work process to verify the medication wasn’t properly followed. Somehow, nurses had been signing off on the chemo medication without verifying the original order. On this day, the certified nurse followed the process. The non-certified nurse was a little annoyed because following the process took precious time away from providing face-to-face care for patients. Why wouldn’t the certified nurse just sign off on the drug? After all, there was nothing new. This medication had already been signed off on by multiple chemo-certified nurses and given to the patient for almost two weeks.
The certified nurse and the non-certified nurse proceeded to look up the original medication order in the chart. When they found the order, they both got a terrible feeling. They realized the medications did not match. They immediately notified the patient’s doctor and the mitigation process began.
Why Did It Happen?
Multiple breakdowns in work processes occurred that led to this incident. The pharmacist misread the medication order. They mistakenly thought the order was for a chemo drug in pill form instead of the antibiotic in pill form. The medications had similar spellings. Also, the medication was not properly verified prior to giving it to the patient the first time. Plus, for two weeks, the subsequent verifications were not properly carried out. It is possible that in an effort to save time, multiple other chemo-certified nurses signed off on the verification without actually comparing the medication delivered to the medication ordered by the doctor. It is possible that each chemo-certified nurse assumed the medication was correct because it was assumed that the medication was checked and verified by the prior nurse and the patient was on in an oncology unit.
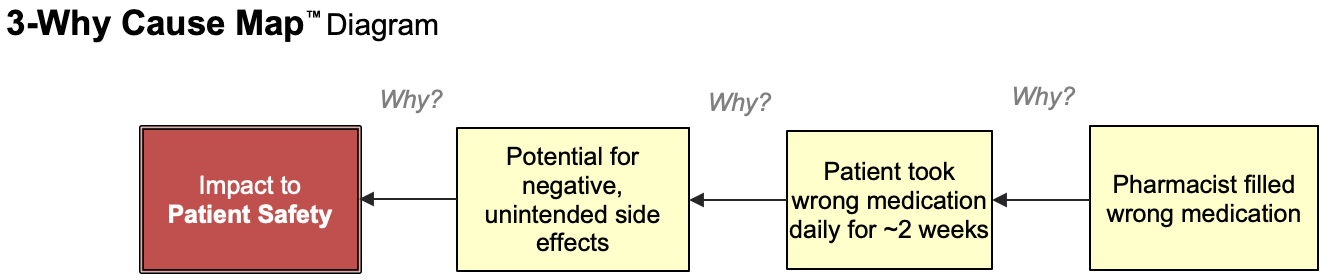
So the fact that there was a chemo medication being used was not out of the ordinary. Many investigators may jump to “human error” as the so-called root cause of the incident. We begin with the impact to the organization’s goal and ask why was there a potential impact to the patient’s safety? The cause is placed in the box to the right. Following this format, we continue to ask Why questions to better understand and Map out the details of the incident. If we begin this way, we may get an accurate, though incomplete, 3-Why Cause Map™ diagram that looks like this:
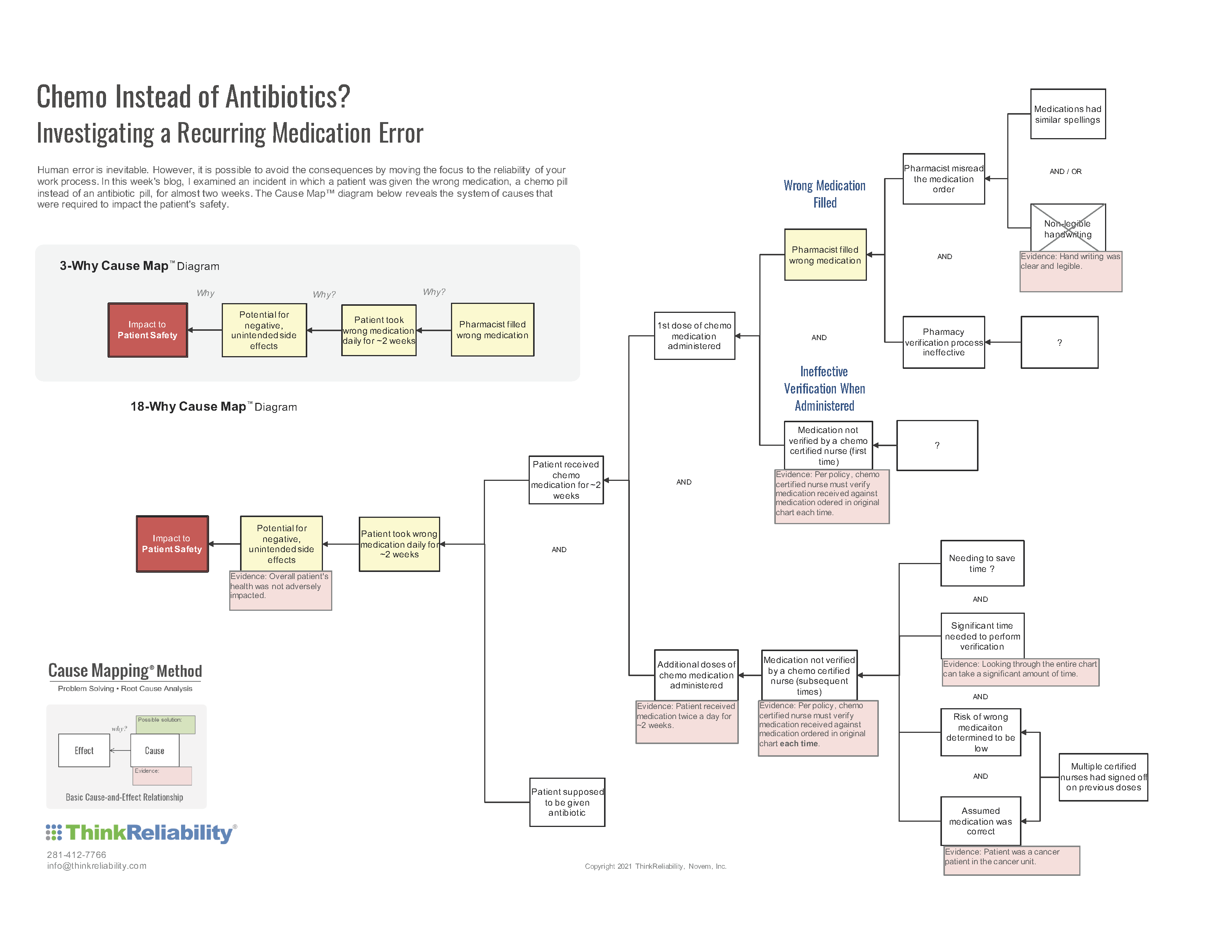
These are a few of the causes of the potential impact to safety. But as you ask more questions, hear additional perspectives of the incident and gather additional evidence, more causes of the incident are uncovered. Below is an example of what a Cause Map diagram with additional detail may look like for this incident. Click on the thumbnail to download the PDF.
Lessons Learned for Work Process Improvements
By breaking an incident down into its causes, we’re able to see more solution options and work process improvements. For example, illegible handwriting used to cause a significant number of medication errors, but since most hospitals and offices have moved to a digital system, those numbers have decreased significantly.
I have quite a few friends who are nurses and sometimes we talk about how the “perfect storm” of causes aligned to lead to an accident. One of my friends agreed to let me use their example as a root cause analysis case study. They were the non-certified nurse in this blog. They told me that they think about this event almost weekly. It serves as a reminder to slow down and follow the process, especially when their first thought is to find a shortcut. We all look for shortcuts and workarounds in our everyday work and home lives.
Let this story be a reminder to slow down and thoroughly consider the risks and unintended consequences beforehand. If you truly found a better, faster, cheaper way to do something, then tell others and evaluate that new work process before implementing it. To learn more about the Cause Mapping method of root cause analysis, check out one of our upcoming trainings.



